Brazil’s Sistema Único de Saúde (SUS) is funded through a tripartite structure shared by municipalities, states, and the federal government, under a web of oversight that follows public money across these different levels of government and even across branches. Spending is audited by the Courts of Accounts at the federal, state, and municipal levels, each responsible for reviewing expenditures within its own jurisdiction, and by the Office of the Comptroller General at the federal level.
Each level of that tripartite structure has a constitutionally required minimum investment in health. Municipalities (including the Federal District) must apply at least 15% of their tax revenue to public health actions and services, while states must apply at least 12%. At the federal level, rules changed with a 2015 constitutional amendment that tied minimum spending to Net Current Revenue (RCL), reaching 15% through transition mechanisms. In practice, the federal government is usually the main funder, but the system only works because the other two levels also invest consistently and keep local services operating.
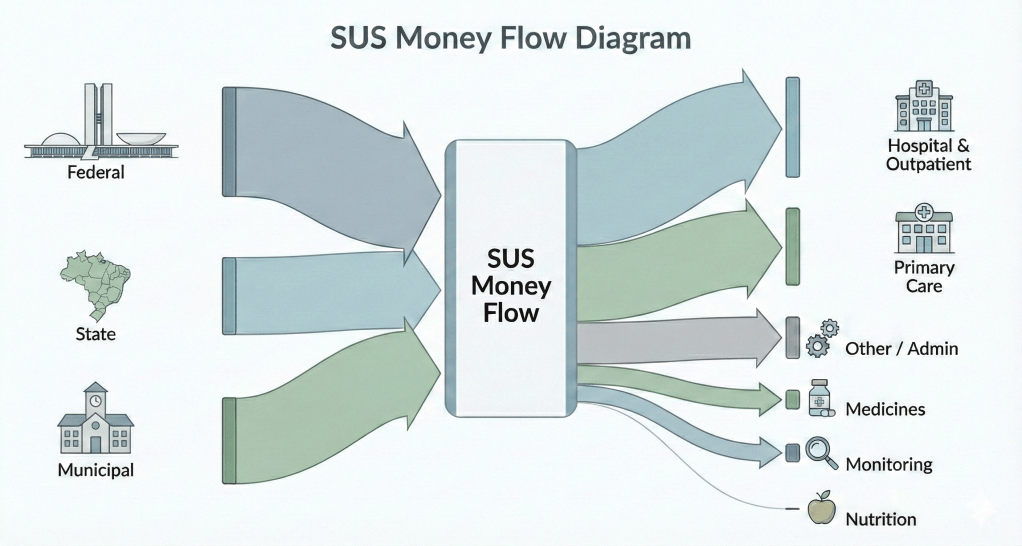
Most federal resources flow from the Ministry of Health through the National Health Fund (FNS) and are then transferred to state and municipal health funds. That structure is not just a technical detail; it is what makes SUS decentralized in real life. It allows municipalities and states to keep UBS clinics open, pay health workers, maintain basic services, and purchase supplies according to local needs. The federal government still concentrates direct purchasing in areas where scale matters, such as vaccines, which are the classic example, through the National Immunization Program, and some high-cost medicines where centralized negotiation can reduce prices. Even so, implementation is largely local: states and municipalities translate national policy into actual service delivery, sometimes using contracted providers depending on the service and the local network.
On the spending side, SUS makes the most sense when you see it as a “complexity pyramid.” At the top, medium, and high-complexity care (MAC) includes hospitals, surgeries, dialysis, intensive care, cancer treatment, and advanced diagnostics. These services tend to absorb the largest share of federal health spending, often around half or more, because unit costs are high. One day, in an ICU, one round of chemotherapy, or a major surgery costs far more than dozens or even hundreds of basic consultations. This is also why MAC spending is usually concentrated in large urban centers and state-level hospital networks, where the infrastructure and specialized staff exist.
At the base of the pyramid is primary care, which includes UBS units, Family Health Strategy teams, community vaccination, and preventive services. Primary care typically takes a smaller portion of the total budget, often in the 15% to 20% range, but it has a strategic role. Strengthening primary care is one of the main ways SUS tries to reduce avoidable hospitalizations and prevent chronic conditions from escalating into expensive emergencies. In recent years, federal transfers to primary care have grown, reflecting this push toward prevention and continuity of care rather than relying on hospitals as the default entry point.
A third area that deserves its own spotlight is pharmaceutical assistance. Medication spending is often described in three layers: basic medicines for common chronic diseases that are distributed through UBS; strategic drugs linked to national programs for conditions such as HIV/AIDS and tuberculosis, which are frequently purchased centrally; and specialized high-cost medications, including biologics and treatments for rare diseases. This last category is especially sensitive because it can expand quickly, and it is also where health litigation often shapes what gets purchased and for whom, sometimes forcing the system to fund therapies outside routine planning.
Instead of seeing SUS as controlled by a single authority, it is more accurate to say it is coordinated through shared rules and negotiated responsibilities across levels of government. Federal guidelines, financing parameters, and national programs create a common direction, but states and municipalities make the system real through local planning, management, and service delivery. This is also why SUS can be both impressive and uneven: it is universal in design but dependent on local capacity in execution.
