A friend of mine got sick in Brazil while visiting from Chile and needed to see a doctor. She went to a “primary health unit” (“Unidade Básica de Saúde,” UBS) where they quickly checked her into the system and directed her to the right line. After a short wait, she had a full appointment conducted in Spanish. The doctor spent more than thirty minutes explaining what was happening in her immune system, why she needed medication, and exactly how long to take it. Afterward, they took her to the pharmacy inside the UBS and handed her the medicines. Then came the moment that shocked her: when she asked where to pay and how much it would cost, the pharmacist told her it was all free, no bill, no charge, because Brazil’s public health system provides care to anyone on Brazilian territory. She couldn’t believe it. “The only thing they asked me to do,” she said, “was rest for the next few days.”
Her experience is not an exception or an act of goodwill, but rather it is how the system is designed to work. Brazil’s public health system, known as SUS for “Sistema Único de Saúde” (Unified Health System), is built on a constitutional promise: Article 196 establishes health as a right and places responsibility on the government to protect it through policies that prevent illness and guarantee access to care.
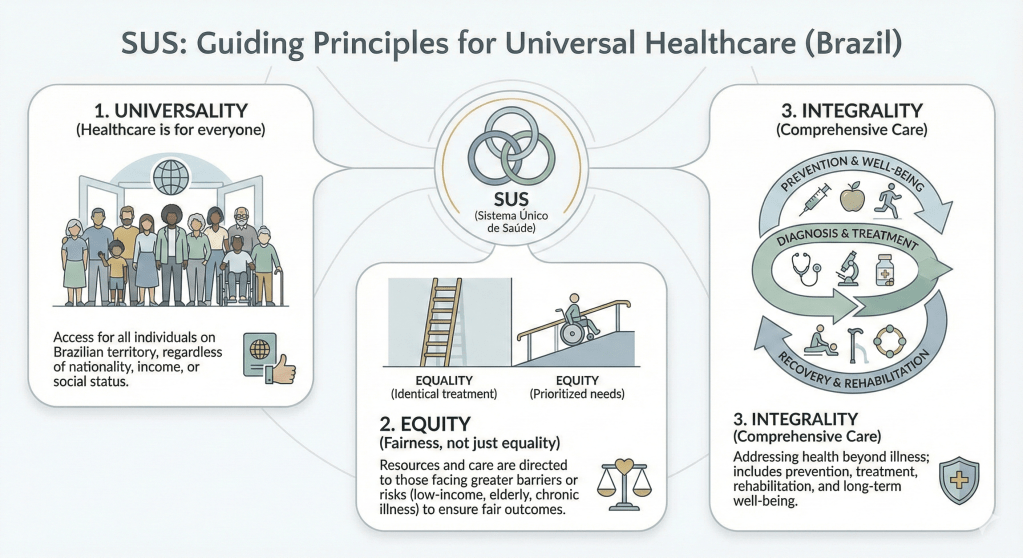
A promise written into law means nothing without the structure to deliver it, which is why SUS operates according to a set of guiding principles that shape how care is actually provided, laid out in the 1990 law that implemented SUS. The first principle is universality: healthcare is for everyone. Whether you’re Brazilian or not, rich or poor, SUS is meant to be available for routine check-ups, hospital visits, or emergencies. The second is equity, which recognizes that equal access does not always mean identical treatment. SUS prioritizes people facing higher barriers or greater health risks: low-income communities, older adults, people with disabilities, those living with chronic illnesses or undergoing cancer treatment, people with HIV, pregnant women, and children. The third principle is integrality, or comprehensive care, which means health is not only about responding to illness: SUS also emphasizes prevention and long-term well-being through vaccination drives, hygiene education, nutrition guidance, environmental protection, and other public health measures designed to reduce disease across the population.
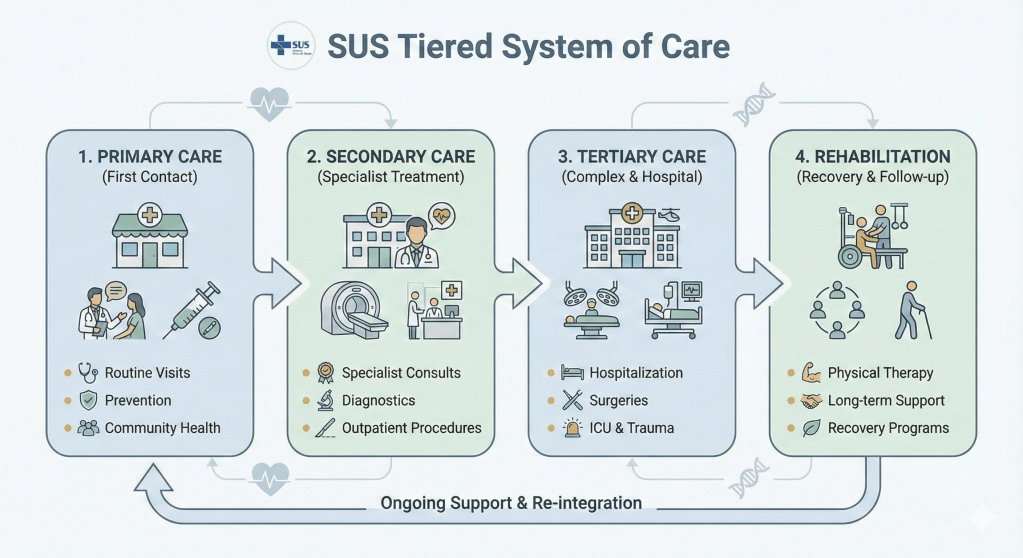
These principles do not exist in the abstract. They take shape through a tiered system of care designed to respond efficiently to different needs. Primary health care serves as the first point of contact and provides direct, ongoing contact with the population through doctor appointments, home visits, vaccination campaigns, awareness programs, and regular community engagement. Secondary care addresses patients with diagnosed or suspected conditions who need specialist evaluation or treatment. Tertiary care handles more complex situations, such as hospitalization, intensive treatments, and ICU support. And rehabilitation provides follow-up and recovery services, often delivered by physical therapists and other specialists.
To deliver care across these different levels, SUS relies on a range of facilities, each serving specific functions within the broader system. Primary health units (UBS), like the one my friend went to, provide ongoing, non-urgent care. Urgent care clinics (“Unidade de Pronto Atendimento”, UPA) handle lower-complexity situations that still require prompt attention. Hospitals manage surgeries and major emergencies. Mobile emergency medical services (“Serviço de Atendimento Móvel de Urgência”, SAMU), the ambulance and paramedic system, provides rapid response and transport. Supporting this network are clinical laboratories for diagnostic testing and research institutions, both government-linked and university-based, that advance treatments, vaccines, and public health knowledge.
What my friend experienced that day was not a fluke. It was SUS functioning as intended, a system designed not just to treat illness but to protect health as a fundamental right. The structure exists because the Constitution demanded it, and the principles guide it because access alone is not enough. Understanding how SUS works helps us see what it means to organize a healthcare system around the idea that no one should be turned away, that care should meet people where they are, and that health is more than the absence of disease: it is something worth protecting for everyone.
